Bluesky Explainer thread by Dr. Kate Kennedy here:
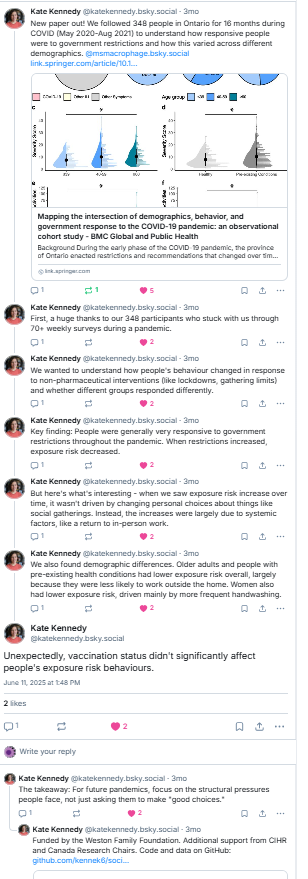

Bluesky Explainer thread by Dr. Kate Kennedy here:
Below is an ‘explainer’ thread from Bluesky. See original here
Publication alert: “No evidence of immune exhaustion after repeated SARS-CoV-2 vaccination in vulnerable and healthy populations” @natcomms.nature.com The backstory is particularly interesting-it’s a tale of the conflicting needs of scientists & decision makers in times of disinformation ….1/n
To begin – my team was funded by the CITF to study COVID-19 infections/vaccinations in older adults & people on immunosuppressants. We had a broad mandate to look at ‘cellular & humoral immunity’ and unlike most grants there was a constant feedback to decision makers, participants & the public 2/n https://www.covid19immunitytaskforce.ca/
This meant that I got a pretty good sense of people’s worries and concerns and we could get solid data to address them. Case in point – we provided data that long-term care residents needed a 3rd dose and then a 4th – they got them and colleagues proved they prevented many infections 3/n https://www.bmj.com/content/378/bmj-2022-071502.short
In 2021 internet personalities were fretting that too many vaccines would lead to ‘immune exhaustion’. Most immunologists were not worried (explanation to follow) but I was shocked to hear in meetings that some folks on decision making tables were worried, esp, for vulnerable populations 4/n
What is this scary ‘immune exhaustion’? When you turn on an inflammatory response (e.g., by vaccination/infection) you have to have a way to turn it off. T cells that recognize an antigen multiply, make cytokines and start to express ‘off-switches’ which have names like PD-1, Tim-3 & Lag-3. 5/n
When there is a lot of antigen around (ie. during infection or vaccination) the balance between the on-switch (antigen-stimulation) and the off-switch (PD-1 & friends) favours being on – the T cells expand & differentiate & work their magic. Here PD1 is better described as an ‘activation marker’….. 6/n
…than an exhaustion marker. When the antigen decreases (ie infection or vaccine clears), the off-switches signal that it’s time to close up the inflammatory shop. It is pretty rare that antigens don’t go away but in cancer that chronic stimulation can lead to sustained expression of the PD1 off-switch. 7/n
How do you know when a T cell is truly ‘exhausted’? It expressed these markers AND it loses its function. Here’s where our study shines – we looked at the T cells’ ability to produce at least 1 cytokine (‘functionality’) or more than 1 cytokine (‘polyfunctionality’). 8/n
Repeat vaccination does not affect the T cells ability to make cytokines, even in vulnerable populations. They may express some activation markers but they are definitely not turned off. 9/n
Pity the lead author, PhD student @jennabenoit.bsky.social Her committee would grill her ‘why are you doing this- we all know vaccines don’t cause exhaustion!’ She held strong “Because policymakers & the public need us to PROVE this in THESE people”-She was strong, thorough & committed. 10/n
So why do so many people make such rash statements on whether a T cell is doing it’s thing (PD-1 = activation) vs crashing out (PD-1 =exhausted)? Above I said this disinformation began circulating in 2021 – we’ve been working on this story since then 11/n
Measuring 1 marker (eg PD1) and making wild inferences is relatively cheap & quick but measuring T cell function and analyzing these complex data is slow & expensive. Indeed we had a team of people working very hard in a clinical trials quality immune testing lab and an analysis team to generate these data. 12/n
https://healthresearch.healthsci.mcmaster.ca/single-cell-spatial-profiling-core-facility/human-immune-monitoring-services/
Learnings: Disinformation = quick to make up but hard to disprove and even immunologists and experts can have seeds of doubt sown by bad actors. Vulnerable populations deserve to be included in research. Negative data studies are impt but hard to sell (see reviews of the paper!). 13/n
Huge shout out to lead author @jennabenoit.bsky.social and the not-on-Bluesky team from our star phlebotomist/blood processor Braeden Cowbrough, flow cytometry genius Dr. Jessica Breznik, analytics guru Dr. Chris Verschoor, and HITS Team (Nichols, Hagerman, Bramson) and of course our participants. 14/14
Dr Bowdish’s solo storytelling/scicom presentation recives a 5N review from Next Magazine! Read the full review here: https://nextmag.ca/fringe-review-the-perils-of-being-born-in-the-fall-provides-laughter-tears-and-scientific-history/

Below is a Bluesky thread that summarizes and explains our manuscript. Click here to read it on Bluesky.
New publication alert! “Reassuring humoral and cellular immune responses to SARS-CoV-2 vaccination in participants with systemic sclerosis” Read on to learn why we did this study and why it is important. 1/n https://www.sciencedirect.com/science/article/pii/S0165247824001032?via%3Dihub
Systemic Sclerosis(SSc) is a rare autoimmune disorder that causes fibrosis of the organs. Because it is caused an immune system gone awry, patients and their doctors were concerned that their immune systems might not respond to the vaccine and leave them less protected 2/n
Because SSC is an autoimmune condition, people generally take immunosuppressive drugs, which can also lead to lower vaccine responses and higher risk of infection. We investigated whether antibody or T cell responses to vaccination were affected in SSC. 3/n
Good news! People with SSC made the same amount of antibodies to the receptor binding domain of the Spike protein (i.e, the bit of the virus that the virus uses to get into us) after their second, third, and fourth SARS-CoV-2 vaccinations. 4/n
More good news! T cell responses to vaccines are thought to help with severe disease and may offer some cross-variant protection. Following the second, third, and fourth SARS-CoV-2 vaccinations, participants with SSc had T cell responses = those without SSC. 5/n
For the immunology geeks: People living with SSc have elevated levels of serum cytokines associated with T cell differentiation. Could this change Th1/2/17/reg mix posts vaccination? Nope. 6/n
Caveat#1: This is a small study (because a rare disease) and we couldn’t investigate all the different drugs that people are on. For more info on how drugs affect vaccination responses see our other studies 7/n https://acrjournals.onlinelibrary.wiley.com/doi/full/10.1002/acr2.11697
Caveat #2: This is very much a comparison of the quantity of immune responses, not the quality. There could still be qualitative differences in immune responses that we didn’t catch but… 8/n
…even though there is very little data on whether SSC is associated with higher infection risk or poorer outcomes what little exists doesn’t find a massive difference compared to the general population 9/n https://acrjournals.onlinelibrary.wiley.com/doi/full/10.1002/acr.25226
Take home message #1: Participants with SSc mount similar responses to SARS-CoV-2 vaccination as controls who do not have autoimmune conditions. 10/n
Take home message #2: Many ppl with autoimmune conditions are afraid that vaccination is unsafe for them because they know their immune system is a bit wonky. It is not the disease that affects immune responses, rather it’s some, not all, drugs at some, not all, doses. 11/n
Thanks to emerging leader & 1st author Jenna Benoit (graduating & looking for a job next year – hint), rheumatologist extraordinaire, Dr. Maggie Larche, cellular immunologist Dr. J. Breznik & J Bramson, team Antibody (Nazy, Huynh) & with special thanks to…..12/n
….our participants. People with SSC often have skin changes which makes blood draws especially hard. Thank you for your commitment to our study and huge props to our exceptional phlebotomist/RC Braeden Cowbrough – our unsung hero. 13/n Fin.
Jenna Benoit (PhD candidate) has published her first, first author paper characterizing how immune responses to vaccination differ in people living with rheumatoid arthritis. We found some interesting new drug-immune interactions.
See thread here: https://bsky.app/profile/msmacrophage.bsky.social/post/3kh2uswvqtm2u
or below….
New paper alert! @jennabenoit.bsky.social and team studied COVID-19 vaccinations in people living with rheumatoid arthritis who are on immunosuppressive drugs and found some interesting, and to our knowledge, unknown effects of specific drugs 1/n
Almost all studies of vaccine immunogenicity (i.e., how strong an immune response is to a vaccine) focus on antibody responses. Measuring the amount of antibodies produced is cheap and (relatively) easy; however, in the Omicron-era these are less predictive of protection than you might think 2/n
When investigating anti-receptor binding domain (RBD) antibodies @jennabenoit.bsky.social and team found that -unsurprisingly- people living with RA and men had lower antibody responses (men have lower antibody responses to vaccination in general), and people with COVID had higher responses (i.e., that hybrid immunity you’ve heard so much about) 3/n
What caused these lower antibody responses? DMARDs (disease modifying anti-rheumatic drugs),and anti-TNF were not associated with lower antibody levels, the effect of steroids was not significant, but costimulation inhibitors reduced antibody levels 4/n
Important caveat: The effect of co-stimulation inhibitors was about the same as being a biologic male, so whether this reduction is associated with increased risk of infection or not is not something we can comment on 5/n.
We didn’t see an effect of drugs on neutralizing antibodies (i.e., antibodies that bind the virus really well and prevent it from entering us), but we did not have enough people on some of the drugs to really investigate this 6/n.
My favourite part: CD4+ and CD8+ T cell responses to vaccination are much, much harder to measure (each dot on the graph costs about $350 and 3+ hrs of time – hence the ‘team’ I keep mentioning) but we know that they are important for preventing infection.7/n
We found that people living with RA had lower CD4+ T cell responses (= ‘helper’ cells that support many aspects of the immune response to infection & vaccination), those who had had COVID were higher – more of that hybrid immunity you’ve heard about. 8/n
BUT even though we had a small number of people on JAK inhibitors, those who were on them had markedly lower CD4+ responses. The effect of co-stimulation inhibitors was not as apparent – but again low numbers of participants so hard to say. 9/n
Speculative side note: We use influenza vaccine as a control. Everyone has had exposure as kids so this measures a memory response made prior to having been vaccinated. Co-stim inhibitors don’t affect influenza but JAK inhibitors do – therefore no defect in pre-drug immune responses? 10/n
CD8+ T cell responses (‘killers’ of virus infected cells), were higher in men (previously known), and didn’t seem to be lower in most drugs, except maybe steroids. 11/n
Caveats: Our study was small and due to the fact we were measuring 1,2,3 doses, we were recruiting fast and furious and didn’t capture as many people on some of the drugs as we would have liked,so all results need to be replicated. 12/n
Clinical relevance: Some of these drugs are associated with increased risk of severe disease (see text for references) and by learning which aspects of the immune response they affect, we learn which aspects of the immune response are required for a successful vaccine. 13/n
Deepest appreciation for our research participants, the Canadian Arthritis Patient Alliance (see website for talks on this topic), the SUCCEED investigator team, our technical staff, fundign from the Public Health Agency of Canada, and you for reading to 14/n
Jessica Breznik (co-supervised by Dr. Deborah Sloboda) won the “Best Presentation by a PhD student” while Pat Schenck (co-supervised by Dr. Mike Surette) won runner up! What a wonderful tribute to their skills in both research and communication – well done!

Congratulations Sara for winning the Gerald T Simons award for her presentation at the Microscopical Society of Canada and Microscopical Society of America (M&M2018) in Baltimore.

To read her award winning abstract, click here.
Congratulations to the newly minted Dr. Loukov on successfully defending her thesis entitled “Age-Associated Inflammation impairs Myeloid Development and Monocyte & Macrophage Function”!

The newly minted Dr. Loukov drinks from the chalice.

Dessi celebrates her thesis defence with one of her mentors Dr. Mark McDermott.

Two doctors.
The Bowdish lab would like to congratulate our latest MSc, Grace Teskey on a great MSc defence. Congratulations Grace!

Grace drinks from the chalic after defending her MSc.
Grace’s words of wisdom.
Congratulations to Melissa Ling, a former Bowdish lab undergraduate thesis student who was accepted to Yale University’s Masters of Medical Science in the Physician Associate Program. This prestigious program has a 3.6% acceptance rate so we are very proud of her.
Best of luck Melissa!
Pictured here in her Bowdish lab days.